21. March 2026
SKIN HEALTH & PHOTOPROTECTION
The Sunscreen You Choose Matters:
An Evidence-Based Guide to SPF
By Lee Hemmings, RN, MRCN, NMC-Registered Advanced Nurse Practitioner in Aesthetics
Whether you are managing post-procedure skin, tackling hyperpigmentation, slowing photoageing, or simply maintaining skin health, the type of SPF you use matters just as much as whether you use one at all. This guide aims to demystify the different formulations available, provide the evidence underpinning their efficacy, and help you make an informed choice suited to your skin.

Why Sun Protection Is Non-Negotiable
Ultraviolet radiation is divided into two clinically relevant wavelengths: UVA (320–400 nm) and UVB (290–320 nm). UVB is responsible for sunburn and plays a key role in the development of non-melanoma skin cancers and melanoma. UVA, which penetrates more deeply into the dermis, causes photoageing — including collagen degradation, pigmentation, and elastin damage — and contributes significantly to carcinogenesis (Narayanan, Saladi and Fox, 2010).
A landmark study by Hughes and colleagues (2013) demonstrated that daily sunscreen use significantly slowed photoageing compared with discretionary use over a four-and-a-half-year period in adults under 55 years of age. The evidence is unequivocal: consistent, broad-spectrum photoprotection is one of the most impactful anti-ageing and cancer-preventative strategies available to us.
CLINICAL NOTE
“Broad-spectrum” means a product protects against both UVA and UVB. In the UK, look for products that carry the EU star rating system (UVA in a circle) alongside their SPF rating. The British Association of Dermatologists recommends a minimum of SPF 30 with 4-star UVA protection for daily use (British Association of Dermatologists, 2022).
What SPF Numbers Actually Mean
SPF — Sun Protection Factor — measures a product’s ability to protect against UVB radiation specifically. It is a ratio: SPF 30 means it takes 30 times longer for UVB to redden protected skin compared with unprotected skin. Critically, this is not a linear scale.

Whilst SPF 50 blocks roughly 98% of UVB rays compared with SPF 30’s 96.7%, the difference narrows substantially beyond SPF 50. The more clinically important factor is consistent application and reapplication. Studies show that most people apply only 25–50% of the recommended 2 mg/cm² dose, effectively halving the SPF they achieve in practice (Autier et al., 2007). A perfectly applied SPF 30 will outperform a poorly applied SPF 50 every single time.
APPLICATION RULE
For the face alone, approximately ¼ teaspoon (1.5 ml) of sunscreen is the recommended quantity. For full-body coverage, around 6 teaspoons (30 ml) should be applied. Reapplication every two hours in direct sun exposure is essential.

TYPE 01 - Mineral (physical) Sunscreen
Active filters: Zinc Oxide (ZnO) · Titanium Dioxide (TiO₂)
Mineral sunscreens contain active ingredients that sit on the skin’s surface and work by reflecting and scattering UV radiation. The two approved mineral UV filters in the UK and EU are zinc oxide (ZnO) and titanium dioxide (TiO₂). These are sometimes referred to as “physical” sunscreens, though this terminology has evolved — both reflect and absorb UV to varying degrees (Smijs and Pavel, 2011).
Zinc oxide is particularly valued in clinical practice for its broad-spectrum coverage across UVA and UVB, including the long-wave UVA I range (340–400 nm), which titanium dioxide alone does not adequately address. Titanium dioxide offers excellent UVB and short UVA II coverage (Pinnell et al., 2000). The two are frequently combined to achieve comprehensive photoprotection.
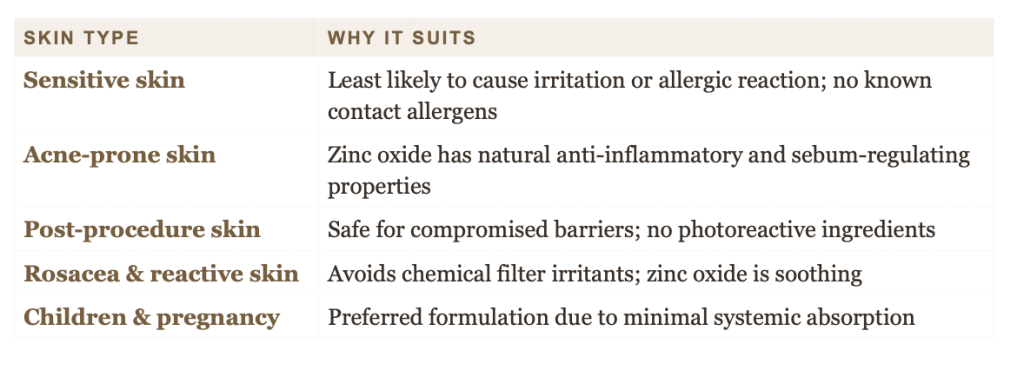
WHY I RECOMMEND MINERAL SPF
Mineral filters are my first recommendation post-procedure — after laser treatments, chemical peels, microneedling, or any treatment that disrupts the skin barrier. They are photostable, begin working immediately upon application, and carry an excellent safety and tolerability profile (Mancebo, Hu and Wang, 2014).
Considerations
The primary clinical drawback has historically been a white cast, particularly on medium to deeper skin tones, owing to the refractive index of these particles. The development of micronised and nano-sized particles has largely addressed this, though concerns around dermal penetration have been raised. Current evidence supports their safety, with the European Commission’s Scientific Committee on Consumer Safety confirming that nano zinc oxide and titanium dioxide do not penetrate healthy or damaged skin to a degree that would raise safety concerns (SCCS, 2021).
Best Suited To
TYPE 02 - Chemical (organic) Sunscreen
Active filters: Avobenzone · Oxybenzone · Tinosorb M & S · Octinoxate
Chemical sunscreens contain organic (carbon-based) UV filters that work by absorbing UV radiation and converting it into heat energy, which is then released from the skin. Common filters include avobenzone, oxybenzone, octinoxate, octocrylene, and the newer generation Tinosorb M and Tinosorb S — widely available in Europe and recognised for their superior photostability and tolerability (Herzog, Osterwalder and Gonzenbach, 2009).
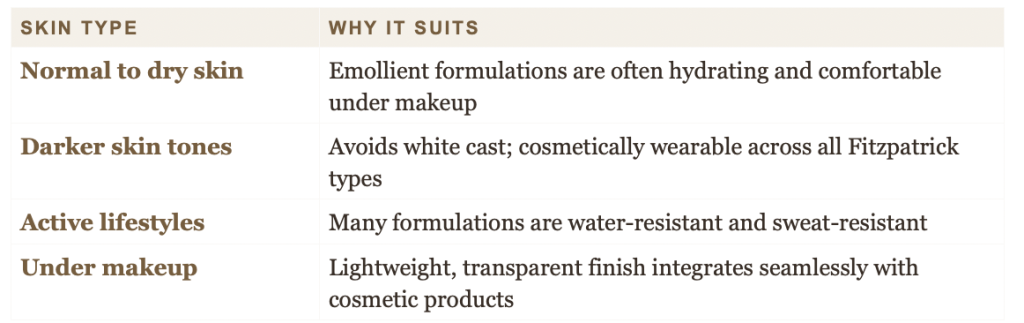
The key advantage of chemical filters is their cosmetic elegance. They absorb readily into the skin, leave no visible residue, and tend to formulate beautifully under makeup. For patients who have historically avoided SPF due to texture complaints, a well-formulated chemical sunscreen is often the product that converts them to daily use.
IMPORTANT CONSIDERATION
Chemical sunscreens require approximately 20–30 minutes to become effective after application, as the UV filters need to bond with the skin’s surface. Application must precede sun exposure accordingly. Some filters — particularly oxybenzone — have raised questions around hormonal disruption in in vitro studies, although regulatory bodies including the EU have set safe concentration limits. Newer-generation filters (Tinosorb S, Tinosorb M, Mexoryl) offer superior photostability and a more favourable safety profile (Gonzalez et al., 2006).
On Melanin-Rich Skin Tones
Chemical sunscreens are particularly well-suited to patients with deeper skin tones, both for the absence of white cast and because the consequences of unprotected UV exposure — post-inflammatory hyperpigmentation (PIH), melasma, and uneven skin tone — are disproportionately impactful for Fitzpatrick skin types IV–VI. Heat generated by chemical filters absorbing UV may theoretically worsen melasma in predisposed individuals; in such cases, a hybrid or mineral formulation may be more appropriate (Sheth and Pandya, 2011).
TYPE 03 - Gel & Fluid SPF Formulations
Formulation types: Water-based · Silicone-based · Hybrid (mineral + chemical)
Gel-based sunscreens are not a separate class of UV filter but rather a formulation type that can contain either mineral, chemical, or a combination of UV filters in a water-based or silicone-based gel vehicle. They merit their own discussion because their unique texture profile addresses a distinct set of clinical needs.
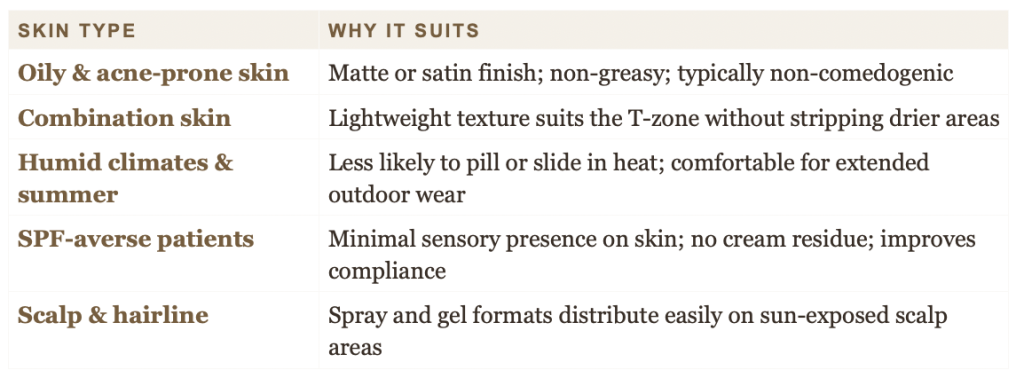
Gel SPFs typically have a high water content, very low to nil oil content, and often contain silicones such as dimethicone or cyclomethicone, giving them a smooth, fast-absorbing, non-greasy finish. They are particularly well-tolerated by oily and acne-prone skin types and are frequently formulated to be non-comedogenic (Bowe and Kircik, 2014).
POST-PROCEDURE USE
Gel formulations with minimal preservatives and fragrance are an excellent option in the early post-procedure phase for patients who find cream or lotion SPFs too occlusive. However, alcohol-containing gel formulations should be avoided on disrupted or sensitised skin, as they can impair barrier repair.
Hybrid Formulations
Many contemporary gel SPFs are hybrid products, combining mineral and chemical filters to achieve broad-spectrum coverage whilst optimising cosmetic acceptability. This approach allows formulators to reduce the concentration of any single filter, potentially improving tolerability, whilst enhancing overall UV coverage. Tinosorb S and M, frequently found in gel and fluid formulations available across Europe, represent a significant advance in this respect (Dario and Arumi, 2019).
Best Suited To
QUICK REFERENCE
Matching SPF to Skin Type
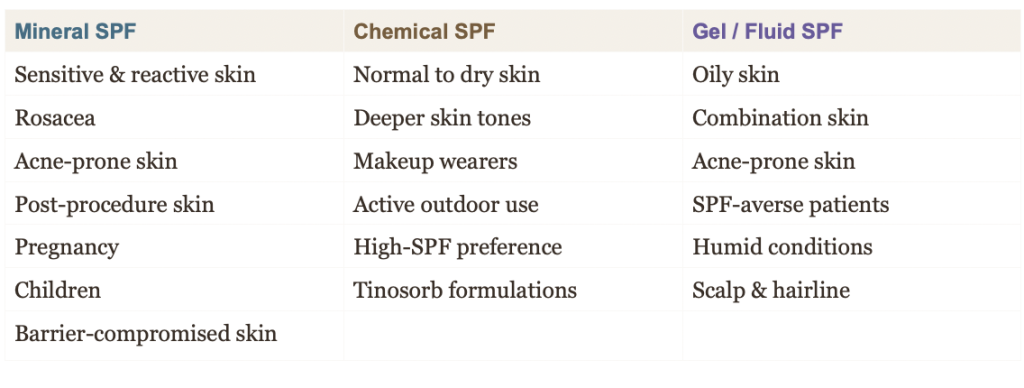
It is worth noting that the best sunscreen is always the one a patient will actually use consistently. In clinical practice, I will often suggest patients trial two or three formulations before committing, as texture preference is one of the principal drivers of compliance (Koster and Berkhout, 2021).

Clinical Guidance & Common Pitfalls
1. SPF Does Not Replace Protective Behaviour
Sunscreen is one component of a comprehensive photoprotection strategy. Seeking shade between 11 am and 3 pm (peak UV index hours in the UK), wearing UPF-rated clothing, and using wide-brimmed hats remain important adjunctive behaviours. Cancer Research UK recommends the combined approach of shade, clothing, and sunscreen — the “SunSmart” framework — for optimal photoprotection (Cancer Research UK, 2023).
2. Vitamin D and Sunscreen Use
A common concern raised in clinic is whether daily SPF use will impair vitamin D synthesis. The evidence suggests that real-world SPF use does not meaningfully compromise vitamin D levels in most individuals (Neale et al., 2019). Patients at risk of vitamin D deficiency should be advised to supplement rather than reduce their sun protection.
3. SPF in Skincare Products vs. Dedicated Sunscreen
Moisturisers and foundations with added SPF are a useful secondary measure but should not replace a dedicated sunscreen as the primary step. The quantity of product applied when using a moisturiser or foundation rarely meets the 2 mg/cm² required to achieve the labelled SPF (Couteau et al., 2012).
4. The Importance of Reapplication
Sunscreen efficacy degrades with time, sweating, sebum production, and rubbing. In outdoor settings or following perspiration, reapplication every two hours is necessary to maintain protection. SPF setting sprays and powder sunscreens offer a practical reapplication method over makeup for many patients.
MY CLINICAL RECOMMENDATION
For the majority of my patients in a UK climate, I recommend a broad-spectrum SPF 50 applied as the final step of a morning skincare routine, before makeup. For patients with oily or acne-prone skin, a fluid or gel SPF will dramatically improve compliance. For those with reactive or post-procedure skin, a mineral-only formulation is my first choice. Above all — find the formulation you will reach for every morning, regardless of the weather.
To see the full range of medical grade SPF - request to join my exclusive skincare store
References
Narayanan, D.L., Saladi, R.N. and Fox, J.L. (2010) ‘Ultraviolet radiation and skin cancer’, International Journal of Dermatology, 49(9), pp. 978–986.
Hughes, M.C.B. et al. (2013) ‘Sunscreen and prevention of skin aging: a randomized trial’, Annals of Internal Medicine, 158(11), pp. 781–790.
British Association of Dermatologists (2022) Sun awareness: advice on sunscreen use. London: BAD. Available at: https://www.bad.org.uk (Accessed: 12 March 2026).
Autier, P. et al. (2007) ‘Quantity of sunscreen applied and the sun protection factor’, Journal of the Academy of Dermatology and Venereology, 21(2), pp. 219–225.
Smijs, T.G. and Pavel, S. (2011) ‘Titanium dioxide and zinc oxide nanoparticles in sunscreens’, Nanotechnology, Science and Applications, 4, pp. 95–112.
Pinnell, S.R. et al. (2000) ‘Microfine zinc oxide is a superior sunscreen ingredient to microfine titanium dioxide’, Dermatologic Surgery, 26(4), pp. 309–314.
Mancebo, S.E., Hu, J.Y. and Wang, S.Q. (2014) ‘Sunscreens: a review of health benefits, regulations, and controversies’, Dermatologic Clinics, 32(3), pp. 427–438.
Scientific Committee on Consumer Safety (SCCS) (2021) Opinion on zinc oxide (nano form) as a UV-filter in sunscreens. European Commission: SCCS/1589/17.
Herzog, B., Osterwalder, U. and Gonzenbach, H. (2009) ‘Broad-spectrum UV-protection by Tinosorb S: an update’, SOFW Journal, 135, pp. 20–24.
Gonzalez, H. et al. (2006) ‘Photodecomposition of the sunscreen agent padimate O into potentially toxic products’, Chemical Research in Toxicology, 19(2), pp. 266–271.
Sheth, V.M. and Pandya, A.G. (2011) ‘Melasma: a comprehensive update’, Journal of the American Academy of Dermatology, 65(4), pp. 689–697.
Bowe, W.P. and Kircik, L.H. (2014) ‘The importance of photoprotection and moisturisation in an antiaging skin care regimen’, Journal of Drugs in Dermatology, 13(2), pp. s25–s32.
Dario, M.F. and Arumi, J.L.R. (2019) ‘New trends in UV protection: development of broad-spectrum and photostable UV filters’, Cosmetics, 6(4), p. 58.
Koster, B. and Berkhout, M. (2021) ‘Determinants of sunscreen use and acceptance among the general population: a systematic review’, International Journal of Environmental Research and Public Health, 18(5), p. 2510.
Cancer Research UK (2023) SunSmart advice: how to enjoy the sun safely. Available at: https://www.cancerresearchuk.org (Accessed: 15 March 2026).
Neale, R.E. et al. (2019) ‘The effect of sunscreen on vitamin D: a review’, British Journal of Dermatology, 181(5), pp. 907–915.
Couteau, C. et al. (2012) ‘Study of the influence of the quantity of sunscreen applied on the sun protection factor’, International Journal of Pharmaceutics, 437(1–2), pp. 250–252.