14. March 2026
Understanding and Treating Acne: A Clinical Perspective
From gentle cleansing to prescription-strength retinoids — what the evidence really says
By Lee Hemmings, RN, MRCN, NMC-Registered Advanced Nurse Practitioner in Aesthetics
Acne vulgaris is one of the most common skin conditions I encounter in clinic. It affects up to 85% of adolescents and a growing proportion of adults — particularly women in their 20s, 30s, and even 40s (Zaenglein et al., 2016). Despite its prevalence, acne is frequently trivialised, and patients often arrive having tried a long line of high-street products with little lasting success. What they need is a clear explanation of what is happening in their skin, and a treatment plan grounded in evidence.
In this blog, I want to walk you through the pathophysiology of acne, explain two of the most effective prescription-level interventions I use — the Obagi CLENZIderm M.D. System and topical tretinoin — and share what the research tells us about why they work.

What Is Acne? The Pathophysiology Explained
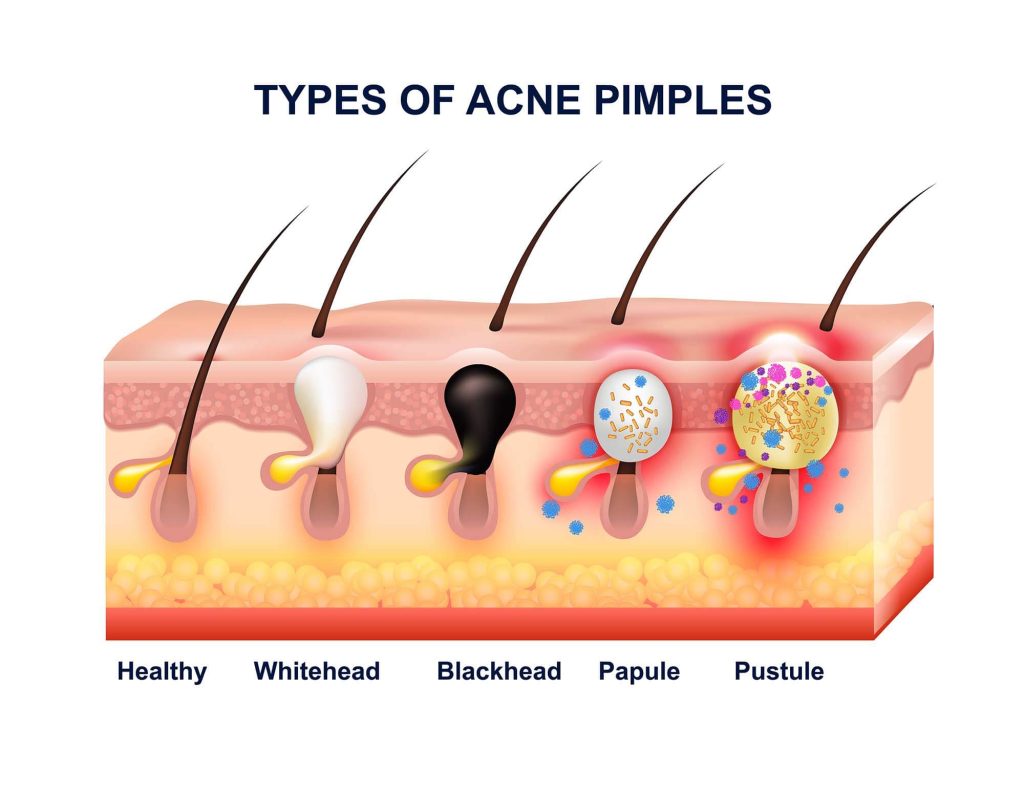
Acne is a chronic inflammatory disease of the pilosebaceous unit — the hair follicle and its associated sebaceous (oil) gland. Its development involves four interconnected processes:
- Excess sebum production, driven largely by androgens
- Abnormal follicular keratinisation, causing the pore lining to shed irregularly and block the duct
- Colonisation and proliferation of Cutibacterium acnes (formerly Propionibacterium acnes)
- Inflammation — both innate and adaptive immune responses triggered by C. acnes and its metabolites
It is worth understanding that the inflammatory cascade begins even before lesions are visible. Recent research using immunohistochemical analysis has demonstrated that subclinical inflammation precedes microcomedone formation (Jeremy et al., 2003). This is important clinically, because it means that treating acne effectively requires targeting multiple pathways — not just tackling visible spots.
Acne is classified by lesion type and severity. Non-inflammatory lesions include open comedones (blackheads) and closed comedones (whiteheads). Inflammatory lesions include papules, pustules, nodules, and cysts. The British Association of Dermatologists (BAD) recommends grading severity as mild, moderate, or severe to guide treatment decisions (Eady et al., 2013).
Clinical Note: Hormonal acne in adult women tends to present in the lower face, jawline, and neck, often flaring cyclically. This pattern warrants consideration of hormonal contributors and may influence treatment choice.

The Obagi CLENZIderm M.D. System
What is it?
The Obagi CLENZIderm M.D. System is a prescription-strength topical regime specifically formulated for mild-to-moderate acne. The system centres on a solubilised 5% benzoyl peroxide (BPO) formulation — a concentration and delivery mechanism that distinguishes it from many over-the-counter BPO products.

How does benzoyl peroxide work?
Benzoyl peroxide is bactericidal against C. acnes through the generation of reactive oxygen species, which disrupt the bacterial membrane and DNA. Crucially, unlike antibiotics, C. acnes has not been shown to develop resistance to BPO — a significant clinical advantage given the rising concerns about antibiotic resistance in acne management (Eichenfield et al., 2013).
BPO also has mild comedolytic and keratolytic properties, helping to unblock follicles, and it has been shown to possess anti-inflammatory effects by inhibiting neutrophil oxidative metabolism (Bojar et al., 1994).

Why solubilised BPO?
Most BPO formulations are suspension-based, meaning the active ingredient sits on top of the skin and can cause significant dryness, bleaching of fabrics, and inconsistent skin penetration. The CLENZIderm system uses a patented solubilised form of 5% BPO, which means the molecule is in true solution. This enhances follicular penetration — delivering the active where it is needed — while reducing surface irritation (Leyden et al., 2008).
A randomised controlled trial by Leyden and colleagues (2008) comparing solubilised BPO with conventional BPO gel found statistically significant superiority in reducing both non-inflammatory and inflammatory lesion counts, alongside better tolerability scores. This aligns with my clinical experience: patients who have previously found BPO-based products drying or irritating often tolerate CLENZIderm considerably better.
The full CLENZIderm regimen
The system is typically used as follows:
- Daily Care Foaming Cleanser (2% salicylic acid) — a beta-hydroxy acid that penetrates the follicle to exfoliate dead skin cells and reduce sebum, preparing the skin for subsequent actives
- Pore Therapy (2% salicylic acid toner) — used to refine pores and continue exfoliation
- Therapeutic Lotion (5% solubilised BPO) — applied to affected areas, targeting C. acnes and reducing comedones
Together, these products address multiple pathogenic factors: excess keratinisation (salicylic acid), bacterial load (BPO), and inflammation (both actives combined). Salicylic acid as a beta-hydroxy acid is lipophilic, meaning it penetrates the sebaceous follicle readily, making it particularly suited to oily, acne-prone skin (Arif, 2015).
Safety Consideration: BPO can cause bleaching of bed linen and towels. Patients should be advised to use white or old fabrics whilst using BPO-containing products. Initial dryness, flaking, or mild erythema may occur in the first one to two weeks and generally settles.
Tretinoin: The Gold Standard Retinoid
What is tretinoin?
Tretinoin (all-trans retinoic acid) is a first-generation topical retinoid and is considered the gold standard in the pharmacological treatment of acne. It is a vitamin A derivative that binds directly to nuclear retinoic acid receptors (RARs), influencing gene expression in keratinocytes — the skin cells lining the follicle.

Mechanism of action
Tretinoin's primary action in acne is normalisation of follicular keratinisation. It accelerates epidermal cell turnover, reduces cohesion between keratinocytes, and prevents the formation of the microcomedone — the earliest, invisible lesion from which all acne develops (Kligman, 1982). By addressing the microcomedone, tretinoin tackles acne at its root.
Beyond this, tretinoin has been shown to:
- Reduce sebum production through effects on sebocyte differentiation
- Modulate the skin's inflammatory response via Toll-like receptor pathways
- Promote desquamation, preventing follicular plugging
- Enhance the penetration and efficacy of other topically applied agents, including BPO and antibiotics (Zaenglein et al., 2016)
This last point is particularly relevant in practice. Tretinoin effectively 'opens' the follicle, making it more accessible to other topical treatments. This is why combination therapy — tretinoin with BPO, for instance — consistently outperforms either agent alone in clinical trials.
The retinisation period
One of the most common reasons patients abandon tretinoin is the initial 'retinisation' period — typically the first four to eight weeks of use — during which the skin may experience dryness, flaking, redness, and a temporary worsening of spots (known as the 'purging' phenomenon). This is normal and represents the accelerated turnover of pre-existing subclinical lesions.
I always prepare my patients for this phase thoroughly. The purge is a sign that the product is working — pushing congestion to the surface — rather than an allergic reaction or sign that the treatment is unsuitable. Most patients who persist through this period report significant improvement by weeks eight to twelve.
The evidence supports this: a systematic review and meta-analysis by Yoham and Casadesus (2023) confirmed that tretinoin produces statistically significant reductions in both inflammatory and non-inflammatory lesion counts compared with vehicle, with continued improvement observed up to twelve weeks and beyond.
How to use tretinoin safely
In my prescribing practice, I follow a 'low and slow' approach:
- Begin with the lowest available concentration (usually 0.025% cream or gel) and increase cautiously
- Apply a pea-sized amount to dry skin, at least 20 minutes after washing — moisture accelerates absorption and irritation
- Start with alternate-night application to build tolerance, moving to nightly use after four weeks
- Moisturise generously — a simple, non-comedogenic moisturiser helps buffer the retinoid effect such as Obagi Hydrate
- Use broad-spectrum SPF 30 or above every morning without fail — tretinoin increases photosensitivity and can worsen post-inflammatory hyperpigmentation without sun protection
Prescribing Note: Tretinoin is a prescription-only medicine (POM) in the United Kingdom. It must only be prescribed following appropriate clinical assessment. It is absolutely contraindicated in pregnancy. Effective contraception must be confirmed before prescribing in women of childbearing potential (MHRA, 2020).
Combining Treatments: The Evidence for Synergy
The most effective acne regimens combine agents that target different pathogenic pathways. The Global Alliance to Improve Outcomes in Acne recommends combination therapy as the standard of care for most patients with moderate acne (Gollnick et al., 2003).
In clinical practice, I commonly use the CLENZIderm system alongside tretinoin. Applied in the morning, the CLENZIderm cleanser, toner, and BPO lotion reduce bacterial load and exfoliate the follicle throughout the day. Applied in the evening, tretinoin normalises keratinisation and drives cellular turnover overnight.
This dual-approach — antimicrobial and keratolytic by day, retinoid-driven at night — addresses all four core pathogenic factors: excess sebum, abnormal keratinisation, C. acnes, and inflammation. Importantly, using BPO and tretinoin together does not cause mutual inactivation when applied at separate times of day, addressing a common misconception (Tanghetti & Popp, 2009).
Patients should be advised that acne treatment requires patience. The British Association of Dermatologists advises allowing a minimum of twelve weeks before assessing treatment efficacy (Eady et al., 2013). Premature abandonment of a regimen is one of the most common causes of treatment failure.
Managing Acne in Melanin-Rich skin
It is essential to approach acne management thoughtfully in patients with darker skin tones (Fitzpatrick skin types IV–VI). Post-inflammatory hyperpigmentation (PIH) — the dark marks left after acne lesions resolve — can be as distressing as the acne itself, and in some cases more persistent.
Both tretinoin and salicylic acid have evidence supporting their use in PIH, making the CLENZIderm and tretinoin combination particularly useful in this population (Davis & Callender, 2010). However, the risk of irritation-induced PIH means that the 'low and slow' approach to tretinoin is even more important. I counsel these patients carefully about avoiding over-exfoliation and the non-negotiable importance of daily SPF.

Niacinamide — available in many over-the-counter serums — has also been shown to inhibit melanosome transfer and can be a useful adjunct in addressing PIH alongside the primary acne treatment (Hakozaki et al., 2002).
Hydroquinone for Post-Inflammatory Hyperpigmentation
Where PIH is a significant concern — and it frequently is in patients with Fitzpatrick skin types IV through VI — hydroquinone remains the most extensively studied and widely used topical depigmenting agent available. It works by inhibiting tyrosinase, the key enzyme in the melanin biosynthesis pathway, thereby reducing the production of melanin within melanocytes (Nordlund et al., 2006). Unlike treatments that address melanin already deposited in the skin, hydroquinone acts at the point of production, making it particularly effective when used early and consistently.
In clinical practice, hydroquinone is typically used at concentrations of 2% to 4%. The 2% concentration is available over the counter in some formulations, whilst 4% is prescription-only in the United Kingdom and is the concentration most commonly prescribed for moderate-to-severe PIH. A landmark study by Taylor and colleagues (2003) demonstrated that 4% hydroquinone cream produced statistically significant lightening of PIH compared with vehicle in patients with melanin-rich skin, with a good tolerability profile when used as directed.
The combination of hydroquinone with tretinoin and a mid-potency topical corticosteroid — commonly known as triple combination therapy — has robust evidence supporting its use in PIH. The most studied formulation is Tri-Luma, which combines 4% hydroquinone, 0.05% tretinoin, and 0.01% fluocinolone acetonide. Grimes (2004) demonstrated significant improvement in PIH severity scores in patients with skin of colour using this formulation over eight weeks. The tretinoin component enhances hydroquinone penetration whilst simultaneously driving epidermal turnover, and the corticosteroid reduces the risk of irritation-induced inflammation — which could paradoxically worsen PIH.
There are, however, important safety considerations with hydroquinone that must be discussed with patients. Prolonged continuous use — typically defined as beyond four to six months — carries a risk of ochronosis, a paradoxical darkening of the skin caused by accumulation of homogentisic acid deposits in the dermis (Charlín et al., 2008). This is rare with appropriately supervised use, but the risk underscores the importance of cyclical prescribing: using hydroquinone for defined treatment periods of eight to twelve weeks, followed by a maintenance phase using alternative depigmenting agents such as azelaic acid, niacinamide, or alpha-arbutin.
As with all depigmenting strategies, the consistent use of a broad-spectrum SPF 30 or above is absolutely non-negotiable. UV exposure directly stimulates melanocyte activity and will counteract the effects of any depigmenting treatment. This is reinforced with every patient at every appointment.
Prescribing Note: Hydroquinone 4% is a prescription-only medicine in the United Kingdom and must only be prescribed following appropriate clinical assessment. It should not be used in pregnancy or breastfeeding. Patients should be counselled on the risk of ochronosis with prolonged use and the absolute requirement for daily sun protection. Avoid use near the eyes or on broken skin.
When to Refer
Whilst a great deal of acne can be managed effectively in an advanced aesthetics setting with appropriate prescribing rights, there are clinical scenarios that warrant referral to a consultant dermatologist:
- Nodulo-cystic or severe inflammatory acne, which may require oral isotretinoin (Roaccutane)
- Acne unresponsive to twelve weeks of topical combination therapy
- Significant scarring — early dermatological intervention can reduce long-term scarring burden
- Suspected acne inversa (hidradenitis suppurativa)
- Features suggesting an underlying endocrine disorder, such as polycystic ovary syndrome (PCOS)
Isotretinoin remains the only treatment capable of producing long-term or permanent remission in severe acne, and referral for this should not be delayed in appropriate patients (Layton et al., 1993).
Final Thoughts
Acne is far more than a cosmetic concern — it carries significant psychological burden, including anxiety, depression, and impaired quality of life (Halvorsen et al., 2011). As advanced practitioners, we have both the clinical tools and the prescribing capabilities to make a real difference.
The Obagi CLENZIderm M.D. System and tretinoin are two of the most evidence-based interventions in topical acne management. Together, they address the full spectrum of acne pathogenesis — from follicular blockage and bacterial colonisation to deep comedonal activity and epidermal regeneration. Used correctly, with appropriate patient education, realistic expectations, and sun protection, they form the backbone of a highly effective acne protocol.
If you are struggling with acne — whether you have tried countless products without success, or you are newly diagnosed — a thorough clinical assessment by a qualified prescriber who specialises in skincare can make all the difference. You deserve a treatment plan that is evidence-based, personalised, and properly monitored.
Start your skin journey today
Click here and request to join my exclusive medical skincare store - Virtual consultations available to get you started on your journey to clearer skin.
References
Arif, T. (2015) 'Salicylic acid as a peeling agent: a comprehensive review', Clinical, Cosmetic and Investigational Dermatology, 8, pp. 455–461. https://doi.org/10.2147/CCID.S84765
Bojar, R.A., Cunliffe, W.J. and Holland, K.T. (1994) 'The short-term treatment of acne vulgaris with benzoyl peroxide: effects on the surface and follicular cutaneous microflora', British Journal of Dermatology, 132(2), pp. 204–208.
Davis, E.C. and Callender, V.D. (2010) 'Postinflammatory hyperpigmentation: a review of the epidemiology, clinical features, and treatment options in skin of color', Journal of Clinical and Aesthetic Dermatology, 3(7), pp. 20–31.
Eady, E.A., Layton, A.M. and Cove, J.H. (2013) 'Acne: more than skin deep', Postgraduate Medical Journal, 79(932), pp. 307–309. https://doi.org/10.1136/pmj.79.932.307
Eichenfield, L.F., Del Rosso, J.Q., Mancini, A.J., Cook-Bolden, F., Rodriguez, D.A., Stein-Gold, L. and Cohen, D. (2013) 'Evolving perspectives on the etiology and pathogenesis of acne vulgaris', Journal of Drugs in Dermatology, 12(9), pp. 1038–1047.
Gollnick, H., Cunliffe, W., Berson, D., Dreno, B., Finlay, A., Leyden, J.J. and Thiboutot, D. (2003) 'Management of acne: a report from a global alliance to improve outcomes in acne', Journal of the American Academy of Dermatology, 49(1 Suppl), pp. S1–S37.
Hakozaki, T., Minwalla, L., Zhuang, J., Chhoa, M., Matsubara, A., Miyamoto, K., Greatens, A., Hillebrand, G.G., Bissett, D.L. and Boissy, R.E. (2002) ‘The effect of niacinamide on reducing cutaneous pigmentation and suppression of melanosome transfer’, British Journal of Dermatology, 147(1), pp. 20–31.
Charlín, R., Barcaui, C.B., Kac, B.K., Soares, D.B., Rabello-Fonseca, R. and Azulay-Abulafia, L. (2008) ‘Hydroquinone-induced exogenous ochronosis: a report of four cases and usefulness of dermoscopy’, International Journal of Dermatology, 47(1), pp. 19–23.
Grimes, P.E. (2004) ‘A microsponge formulation of hydroquinone 4% and retinol 0.15% in the treatment of moderate to severe facial hyperpigmentation: efficacy and tolerability in 40 subjects’, Journal of Drugs in Dermatology, 3(6), pp. 651–654.
Halvorsen, J.A., Stern, R.S., Dalgard, F., Thoresen, M., Bjertness, E. and Lien, L. (2011) ‘Suicidal ideation, mental health problems, and social impairment are increased in adolescents with acne: a population-based study’, Journal of Investigative Dermatology, 131(2), pp. 363–370.
Jeremy, A.H., Holland, D.B., Roberts, S.G., Thomson, K.F. and Cunliffe, W.J. (2003) 'Inflammatory events are involved in acne lesion initiation', Journal of Investigative Dermatology, 121(1), pp. 20–27.
Kligman, A.M. (1982) 'An overview of acne', Journal of Investigative Dermatology, 62(3), pp. 268–287.
Layton, A.M., Stainforth, J.M. and Cunliffe, W.J. (1993) 'Ten years' experience of oral isotretinoin for the treatment of acne vulgaris', Journal of Dermatological Treatment, 4(Suppl 2), pp. S2–S5.
Leyden, J.J., Wortzman, M. and Baldwin, E.K. (2008) 'Antibiotic-resistant Propionibacterium acnes suppressed by a benzoyl peroxide cleanser 6%', Cutis, 82(6), pp. 417–421.
Medicines and Healthcare products Regulatory Agency (MHRA) (2020) Isotretinoin (Roaccutane): updated recommendations. London: MHRA. Available at: https://www.gov.uk/drug-safety-update/isotretinoin-roaccutane-updated-recommendations (Accessed: 1 March 2025).
Nordlund, J.J., Boissy, R.E., Hearing, V.J., King, R.A., Oetting, W.S. and Ortonne, J.P. (eds.) (2006) The Pigmentary System: Physiology and Pathophysiology. 2nd edn. Oxford: Blackwell Publishing.
Taylor, S.C., Cook-Bolden, F., Rahman, Z. and Strachan, D. (2003) ‘Acne vulgaris in skin of color’, Journal of the American Academy of Dermatology, 49(3 Suppl), pp. S98–S106.
Tanghetti, E.A. and Popp, K.F. (2009) ‘A current review of topical benzoyl peroxide: new perspectives on formulation and utilization’, Dermatologic Clinics, 27(1), pp. 17–24.
Yoham, A.L. and Casadesus, D. (2023) 'Tretinoin', in StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. Available at: https://www.ncbi.nlm.nih.gov/books/NBK557478/ (Accessed: 1 March 2025).
Zaenglein, A.L., Pathy, A.L., Schlosser, B.J., Alikhan, A., Baldwin, H.E., Berson, D.S., Bowe, W.P., Graber, E.M., Harper, J.C., Kang, S., Keri, J.E., Leyden, J.J., Reynolds, R.V., Silverberg, N.B., Stein Gold, L.F., Tollefson, M.M., Weiss, J.S., Dolan, N.C., Sagan, A.A., Stern, M., Boyer, K.M. and Bhushan, R. (2016) 'Guidelines of care for the management of acne vulgaris', Journal of the American Academy of Dermatology, 74(5), pp. 945–973.
Disclaimer: This blog is written for educational purposes and reflects the clinical experience and professional opinion of the Nurse Lee. It does not constitute medical advice. Tretinoin is a prescription-only medicine and must only be obtained via a qualified prescriber following appropriate consultation. Always seek the advice of a qualified healthcare professional regarding any medical condition.